Last week we discussed the physiology of ethylene glycol poisoning. Treatment is based on understanding that physiology.
Treatment
The goal of antidotal therapy is to prevent the metabolism of ethylene glycol to its toxic metabolites. This is done by blocking the enzyme alcohol dehydrogenase. The parent compound (ethylene glycol) is then slowly excreted via the kidneys.
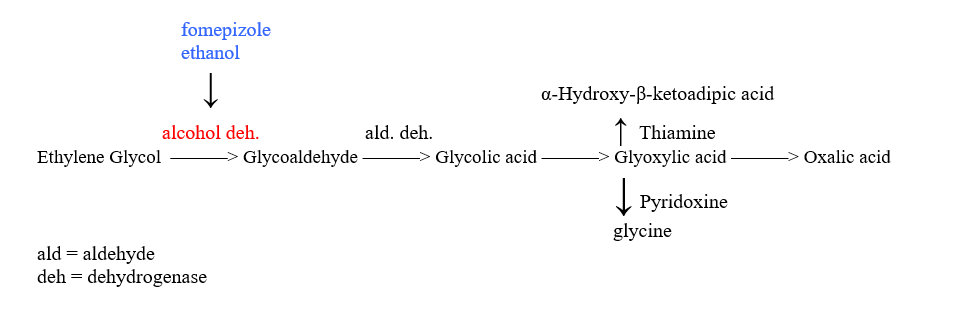
There are two agents available that block alcohol dehydrogenase-ethanol and fomepizole. Both are administered intravenously. Intravenous absolute ethanol effectively blocks alcohol dehydrogenase if the ethanol concentration is greater than 100 mg/dL. Ethanol concentrations must be measured hourly. Remember, ethanol affects sensorium (and reason) and decreases serum glucose. (Call the Poison Center for dosing)
Fomepizole is a potent alcohol dehydrogenase inhibitor and is approved by the FDA for treatment of ethylene glycol poisoning. It has the advantage that it does not affect sensorium or glucose, it is easier to administer as you don’t need to monitor serum concentrations, and it has a longer duration of action. The disadvantage is the price. It costs about $1000/dose.
There is great debate about the benefits of fomepizole due to the cost. There have been no trials comparing ethanol and fomepizole. It is difficult to keep ethanol levels above 100 mg/dL-by the time you receive a lab value that indicates the ethanol is not > 100, change the IV ethanol rate and recheck the ethanol, 2 hours have passed. Furthermore, drunken ICU patients are difficult to manage. I think fomepizole is worth the cost. (You don’t have to worry about harming the kidneys when the ethanol concentration decreases to less than 100 mg/dL)
The indications for administration of the antidote are ethylene glycol levels > 20 mg/dl or an osmolar gap > 10mosm. Antidote administration is also recommended if two of the following are present:*
Arterial pH< 7.3
Serum bicarbonate < 20 mEq/L
Osmolar gap >10
Urinary oxalate crystals present
*(J Tox Clin Tox 1999;37:537-60)
Remember that the antidote is indicated only if there is an osmolar gap. If there is no gap, ethylene glycol is not present and administering the antidote would be of no value.
Cofactors such as pyridoxine and thiamine are involved in the metabolism of ethylene glycol. These are frequently administered although there is no evidence that supplementing these cofactors is effective. Administration of these cofactors should be considered in the alcoholic or vitamin deficient patient.
Seizures can be treated with benzodiazepine followed by Phenobarbital.
Sodium bicarbonate may be administered for the acidosis, but this acidosis does not respond well to bicarbonate alone.
Hemodialysis should be considered if the ethylene glycol level is > 50 mEq/L and in those patients with renal insufficiency/failure. Both alcohol and fomepizole are dialyzable so administration of these agents must be increased.
Considerations
Do not wait for symptoms to initiate treatment.
Patients who present hours after their ingestion may have metabolized the glycol. In this case, there will be a profound acidosis and no osmolal gap.
Indications for treatment can be determined by the presence of an osmolal gap. If there is no gap, treatment is not indicated because the ethylene glycol has already been metabolized.
To calculate the osmolar gap, blood for analysis of osmols must be obtained at the same time as the blood for the electrolytes.
If you do not have intravenous absolute ethanol and are transferring the patient, oral alcohol should be considered.
The Poison Specialists who answer the hotlines (RN, Pharm D, MD) are very adept at helping manage ethylene glycol patients. There is always a MD toxicologist on call, if you wish to speak to a physician.
I am interested in any questions you would like answered in the Question of the Week. Please email me with any suggestion at Donna.Seger@Vanderbilt.edu.
Donna Seger, MD
Medical Director
Tennessee Poison Center