-
Question of the Week
March 16, 2015
What exposures occur during refining?
Crude oil is a complex mix of hydrocarbons benzene, sulfur, nitrogen, chromium, toluene, and xylene. Crude oil is used to make fuel and other petroleum products and is refined to produce gasoline. It is during the refining process that exposures occur that can cause toxicity.
Workers can be exposed to toxins during drilling, pumping, treating, transport by pipeline, ship, rail, and storage. For example, volatile components at well heads, pumps, or through vents in storage tanks and ship’s tanks, create a potential for exposure via inhalation. Crude oils with high concentrations of sulfur can result in inhalation of hydrogen sulfide gas, particularly in confined spaces, well head and storage tanks. Inhalation of benzene, toluene, and xylene can also occur. Human epidemiology data revealed inadequate evidence for carcinogenicity, and therefore crude oil is not classified as carcinogenic.
Typically, crude is transferred to a refinery distillation unit (see diagram below) that separates the crude into different petroleum products. During these processes, carbon monoxide, polycyclic aromatic hydrocarbons (PAH), petroleum asphalt, petroleum coke, chlorine, chromium, and other products are produced and are potential toxins.
Petroleum products have negative impact on the environment and on human health. As petroleum products burn as fuel, they emit gases into the atmosphere, which are potential sources of global warming. Some of these gases emitted include carbon dioxide, carbon monoxide, sulfur dioxide, nitrogen oxides, volatile organic compounds, and particulate matter.
Petroleum industry operations cause a variety of exposures. The chemicals and chemical mixtures have not been fully characterized for their potentially adverse health effects in workers. There is no evidence of significantly increased risk of cancer in petroleum refinery workers. Non cancer exposures cause skin irritation, skin sensitization, and dermatitis.
References
- Work Safe: Occupational Disease Hazards in the Oil and Gas Industry. http://www2.worksafebc.com/i/posters/pdfs/2013/ws_2013_02.pdf
- National Institute of Health: Crude Oil. http://toxtown.nlm.nih.gov/text_version/chemicals.php?id=73
- Environmental Protection Agency: Addressing Air Emissions from the Petroleum Refinery Sector. http://www.epa.gov/eogapti1/video/10182011Webinar/101811webinar.pdf
- United States Department of Transportation: Fact Sheet: Refineries. http://primis.phmsa.dot.gov/comm/FactSheets/FSRefinery.htm
This question prepared by: Elmang Nchako, MD, MPH (Occupational Medicine Resident-PGY 3) Department of Family and Community Medicine Meharry Medical College
-
Question of the Week
February 2, 2015
Is RADON poisonous?
Recently I was interviewed by a television newscaster regarding radon because a couple had become concerned when they were told their dwelling contained a “high amount of radon”. Everyone has questions about radon.
As uranium-238 (naturally occurs in earth’s crust) decays, it forms radon, a gas which “leaks” out of the earth’s crust into the atmosphere. The problem occurs when radon gas gets trapped in buildings: basements, rooms, etc., where it can’t vent or slowly vents into the atmosphere. Radon gas, with its short half-live (~3.8 days), and because it is a noble/inert gas is not a poison itself. There are no immediate signs/symptoms from radon exposure. It cannot be seen, felt, smelled or tasted. It is a heavy gas and tends to accumulate in basements and low areas. Because of the natural radioactive element decay, radon eventually forms radioactive “daughter products” such as polonium 210 (138 day half-live) and 218 (3 minute half-live), and lead 214 (stable nuclide). These latter decay products have much longer half-lives and are potent alpha particle (helium nucleus) emitters. This means a person’s lung alveolar cells get bombarded with alpha particles. Over a life-time, the amount of radon gas trapped in a dwelling where one resides as well as the total amount of radon a person breaths determines their chance of developing lung cancer. Significant exposure to radon over years increases the chance of lung cancer developing.
January is National RADON Action Month. Check out www.epa.gov/radon for more information, and please check your homes, and encourage your patients to check their homes. Many more answers to how to remediate a home are available through this link.
Radon Risk If You've Never Smoked:
Radon Level
If 1,000 people who never smoked were exposed to this level over a lifetime*...
The risk of cancer from radon exposure compares to**...
WHAT TO DO:
20 pCi/L
About 36 people could get lung cancer
35 times the risk of drowning
Fix your home
10 pCi/L
About 18 people could get lung cancer
20 times the risk of dying in a home fire
Fix your home
8 pCi/L
About 15 people could get lung cancer
4 times the risk of dying in a fall
Fix your home
4 pCi/L
About 7 people could get lung cancer
The risk of dying in a car crash
Fix your home
2 pCi/L
About 4 people could get lung cancer
The risk of dying from poison
Consider fixing between 2 and 4 pCi/L
1.3 pCi/L
About 2 people could get lung cancer
(Average indoor radon level)
(Reducing radon levels below 2 pCi/L is difficult.)
0.4 pCi/L
(Average outdoor radon level)
Note: If you are a former smoker, your risk may be higher.
* Lifetime risk of lung cancer deaths from EPA Assessment of Risks from Radon in Homes (EPA 402-R-03-003).
** Comparison data calculated using the Centers for Disease Control and Prevention's 1999-2001 National Center for Injury Prevention and Control Reports.This question prepared by: John Benitez, MD, MPH Medical Toxicologist
-
What do you need to know about Carbon Monoxide (CO) exposure?
This is a topic we discuss every year because CO exposure has potential for devastating sequela.
At one time CO was thought to simply occupy a place on the hemoglobin molecule (carboxyhemoglobin) and create a functional anemia. Unfortunately, CO has additional mechanisms of toxicity. CO shifts the oxyhemoglobin dissociation curve to the left, so that hemoglobin holds onto oxygen much tighter, reducing the amount of oxygen released to the tissues. CO also causes a malfunction of cytochrome oxidase (oxidizing enzyme in mitochondria which transfers electrons from cytochromes to oxygen molecule) which may last for up to three days after a single exposure. The organ systems most impacted by CO exposure are the heart and nervous system.
The symptoms of CO poisoning are nonspecific. Headache, myalgia, and dizziness may be initial symptoms. Cerebral impairment, confusion, coma and death may subsequently occur. One of the consequences of exposure to CO may be delayed (or persistent) neuropsychological sequela which includes memory and concentration impairment, loss of executive function, decrease in IQ, personality changes, neurologic deficits (such as incontinence) and symptoms of Parkinsons syndrome. The problem is neither the carboxyhemoglobin (COhgb) concentration nor the clinical presentation at the time of evaluation predicts who will develop this sequelae.
Studies are conflicting regarding the efficacy of hyperbaric oxygen (HBO) and/or normobaric oxygen in preventing or improving this syndrome. There is the possibility that HBO may increase CNS free radicals-although the clinical implications of this are unknown. There are no conclusive studies. There is agreement that HBO is a reasonable treatment for pregnant women as fetal hemoglobin has a higher affinity for CO than adult hemoglobin. Tennessee Poison Center recommends HBO for pregnant women. For other significant exposures, TPC usually recommends NBO for at least 12 hours, sometimes longer.
Recommendation: In cases of CO exposure, call the Poison Center, document that you called the PC and their recommendations. These recommendations will vary between poison centers. Know what your PC recommends. AND tell all your patients to have a CO detector in their house. Prevention of the exposure is easier than treatment of the sequelae.
This question prepared by: Donna Seger, MD Medical Toxicologist
-
Question of the Week
March 10, 2014
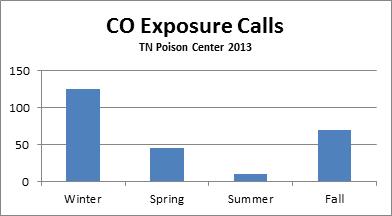
Does CO poisoning occur only during winter?
This Question of the Week was prepared by Bhavana C. Anand, MD, MPH, an occupational medicine resident from Meharry who is spending time with Dr. Benitez.
The answer is No! Carbon Monoxide (CO) poisoning occurs throughout the year.
Over 250 calls related to CO exposure were received by Tennessee Poison Center during 2013. Peak calling rates were in winter and fall.
CO can be produced anytime by burning fuels and inadequate ventilation. Some household examples are furnaces, ovens, idling cars with improper ventilation and water heaters. As CO is a colorless and odorless gas, people don’t recognize the exposure.
During winter, heaters are put back into use, and many people have not done preventive maintenance on their furnaces. They are unaware if the furnaces are adequately functioning or if there is a malfunction with improper ventilation that can lead to CO accumulation inside the dwelling. Water heaters are potentially dangerous when malfunctioning and when used for indoor swimming pools, may again cause CO exposure. . Use of generators indoors or in semi-enclosed areas or fireplaces with improper venting can cause lethal concentrations of CO.
As spring arrives, people get their lawn mowers, tillers, leaf blowers and other gasoline powered machinery out of hibernation. Since it is still cold outside, “quick checks” are sometimes done in a closed or semi-enclosed garage which can be dangerous. Sporadic episodes of cold weather in spring make people reach for their heat sources to warm up the house. This can lead to dangerously high levels of CO in the working area or house if not adequately ventilated. Spring storms bring power outages enticing some people to bring gas powered generators indoors without properly venting them.
In summer, we are out of the cold weather finally and want to be outside. How can being outside predispose you to CO poisoning? It is counter intuitive but some of the fun activities like camping, boating and water skiing can be dangerous. Boats can cause dangerously high levels of Carboxy hemoglobin (COHB) in just minutes. Some boats have generators or motors venting in the rear of the boat; this is a typical spot to place platforms or swim decks. Children who play on these decks or swim under the platforms can be exposed to very high levels of CO. People camping in trailers and tents often cook inside their shelter or use generators to warm these units exposing them to CO.
In fall, cooler weather and cold snaps occur which leads to the same scenario as spring. Leaf blowing and yard maintenance using gas powered units may cause CO poisoning if improperly tested, used, or vented.
All CO accidents and deaths are preventable! CO poisoning can occur throughout the year . . . we should educate our patients at every opportunity. Remind them that ANYTHING that burns a fuel can produce CO gas and may cause poisoning.
Links on CO:
-
Question of the Week
March 4, 2014
Should dental amalgams be removed due to the concern for mercury toxicity?
Mercury is found in the earth’s crust and is ubiquitous in the environment, so most people have small, measurable amounts of mercury that can be detected in their urine, regardless of whether they have mercury containing amalgams. . However, people with mercury containing amalgams often have slightly higher concentrations of mercury in their urine than those without amalgams. Greatest exposure to mercury occurs during the placement or removal of dental restorations. Once the reaction is complete, far less mercury is released. The amount of mercury released varies with the number of restorations, their surface area, mastication, eating habits and tooth brushing habits etc. Dissolution of mercury from the amalgam does occur and mercury is released as metal ions (which passes into oral fluids and ingested) or evaporates as mercury vapor. Mercury vapor in the oral cavity is either exhaled or inhaled into the respiratory system and distributed by blood to the toxicologically sensitive central nervous system and kidneys. It is excreted by the kidney, sweat and saliva. The concentration remains very low and clinically insignificant.
There are concerns with removing amalgams. One is that the mercury in the amalgams becomes more available for absorption into the body during the removal process. Another is that unnecessary removal of the amalgams subjects the person to risks associated with the procedure, such as those from anesthesia, and to the high costs associated with the procedure. And although dental amalgam removal does lead to reduced mercury concentrations in blood and urine, no differences have been observed in organ function or significant effect on general health. There is lack of evidence of improved health outcomes following removal of dental amalgam fillings.
It is important to remember that whatever the substance, development of poisoning depends on the dose to which one is exposed. In the case of mercury, the amount to which a person is exposed simply from having dental amalgams is just not enough to produce harm. The best thing to do is just leave them alone, unless there is another reason for having the amalgams removed.
The American College of Medical Toxicology has issued a recommendation/commentary based on review of scientific evidence which states: Don’t remove mercury-containing dental amalgams.
This question prepared by: Donna Seger, MD Medical Toxicologist
-
Question of the Week – UPDATE
January 14, 2014
To clarify the event in West Virginia: the chemical release was UPSTREAM of the main water intake valve to the region’s water treatment plant. Therefore, the regional water supply was contaminated.
Since yesterday: The “Do Not Use” water order has been lifted from many customers, but as of the morning of 1/14/2014 about 74,000 customers still are being directed not to use the water. Those that can use their water are being told to properly flush their plumbing system prior to using water.
The Elk River flows into the Kanawha (an Ohio River tributary) upstream from Cincinnati, OH. The water treatment plant in Cincinnati is monitoring the situation and is prepared to shut down Ohio River intakes and supplement water from a different water treatment plant that would not be affected by the water contamination. Several other towns in Ohio and Kentucky are prepared to shut water intake from the Ohio River as a precaution.
So far, no fatalities are reported. 234 patients have been treated and released and at least 14 individual have been admitted. Many restaurants remain closed, but many have been approved to open once specific conditions are met. Schools are open in 5 out of the 9 counties affected.
The West Virginia Poison Center continues to receive calls from the public and healthcare professionals. The number of calls regarding the incident over the past 4 days is almost quintupled compared to their routine calls, which of course have continued.
This question prepared by: John G. Benitez, MD, MPH Medical Toxicologist
-
Question of the Week
January 13, 2014
Is the water in West Virginia safe to drink?
In West Virginia on January 9.2014, a “very large release” of a chemical occurred on the Elk River 1.5 miles from the water company’s main intake valve ( area where water is taken from the river , purified and then distributed to city) . This water intake delivers purified water to 300,000 people living in Charleston and the surrounding 9 counties. Seven hours after the “release”, the official “do not use the water” notice was circulated to the public. Reports from the public stated that the air and water smelled like licorice. 4-Methylcyclohexane methanol was identified as the chemical; it is used in the coal flotation process to wash the coal. Toxicity of the chemical is unknown.
The WV poison center received calls about the chemical from the public and healthcare providers. Poison center staff on leave was called back to work because of the increased call volume. Most calls were about human exposure but many calls contained questions about animal exposures. Over 3 days the Poison Center received over 1000 calls related to human exposures, 70 calls related to animal exposures, and over 200 information calls about the chemical, in addition to their normal call volume. The poison center has been working in partnership with all hospitals to provide and collect information, and working with the state and local health authorities to provide appropriate information and triage patients. Several l hospital Emergency Departments evaluated patients exposed to the water. On the 2nd day of the incident, all hospitals in WV were required to report any incident-related admissions to the WV poison center.

The chemical spill has impacted everyone, as water can’t be used for washing, drinking, or bathing. Several restaurants and businesses have closed; hospitals are conserving/rationing water. People must obtain bottled water and drinks. There is no way to rid the water of this chemical.
Further information in future Question of the Week.
This question prepared by: John G. Benitez, MD, MPH Medical Toxicologist
-
Question of the Week
January 21, 2013
What was the role of Tennessee Poison Center in the recent mass exposure of school children to carbon monoxide?
In the late morning of Monday, January 14, Drexel School was closed due to the concern of a carbon monoxide (CO) leak. Initially, the parents were not sure why there had been an early school closure, but the school subsequently sent a telephone announcement alerting the parents that the children had been exposed to carbon monoxide. Parents began flooding to local Emergency Departments (ED).
Tennessee Poison Center (TPC) received a call around noon asking what one should do if one was exposed to carbon monoxide, but an actual exposure was not relayed. A couple of hours later, TPC received a call from Vanderbilt Pediatric Emergency Department regarding a number of children that were presenting to the ED from Drexel School. The likelihood was that there would be many more.
There are a number of issues that need to be addressed in this setting. First is ensuring that the patients are evaluated and treated. Once the exposure is known, then an assessment must be made to determine if the hospital has the required resources to treat these patients. This allows for triage of patients to the hospitals that have the available resources. The treatment for CO exposure is oxygen, and since all hospitals have the ability to confirm exposure to CO and have oxygen, the patients can be distributed throughout hospitals in the community. This distribution prevents one or two hospitals from becoming overwhelmed and other ED patients can still get adequate care.
The media, already on standby, assisted in getting the message to the community. They transmitted the message that if the child did not have symptoms, families should call the Poison Center to determine if he/she needed to go to the ED. If you were going to take your child to the Emergency Department, call the Poison Center to determine which hospital you should attend. Thus, many ED visits were avoided altogether and hospitals throughout the city received the patients, preventing a few hospitals from being overloaded with patients.
At TPC, the Certified Specialists in Poison Information, nurses, doctors and pharmacists who answer the hotline phones, rose to the challenge. They responded to more than one hundred calls regarding carbon monoxide (in addition to the usual calls) over the next few hours.
Not only does Tennessee Poison Center help in an everyday poison emergency, we are ready to respond in any type of disaster involving poisons. When things work well, and a disaster is avoided, it is easy to overlook the efforts that made things work so efficiently and effectively. Whew!
This question prepared by: Donna Seger, MD Medical Toxicologist
-
Question of the Week
April 9, 2012
What is Radon and why does it matter to human health?
Radon (222Rn) is an element, formed as the sixth element in the radiation decay sequence of uranium (238U). It is odorless, colorless and radioactive. Radon itself is not toxic because of its chemical or radiological characteristics! So why worry? Radon continues to decay into several progeny, frequently called “daughter products”; its half-life is about 3.8 days. The progeny, polonium (218Po and 210Po) and lead (214Pb) however emit alpha radiation (helium nuclei) which is toxic to the lung causing increases in small cell and squamous cell carcinomas. The CDC estimates that it is the second leading cause of lung cancer in the US. The EPA and Surgeon General’s office estimate more than 20,000 lung cancer deaths each year are attributable to radon.
Testing homes for radon helps identify homes where radon collects. Since radon comes from the ground it will seep and accumulate into enclosed areas such as basements, buildings, and mines. Radon enters the home through cracks in solid floors and walls, construction joints, gaps in service pipes, cavities in walls, and the water supply. Test kits can be bought that will measure the amount of radon in a home. There are also qualified testers that can come to your home and measure for you. If radon levels are elevated in the home (>4pCi/L), then sealing cracks and joints and possibly installing a radon vent pipe system are indicated. Consult with a qualified or state certified radon contractor. Many states are now requiring radon tests prior to sale of homes.
This question prepared by: John Benitez, MD, MPH Medical Toxicologist
-
Question of the Week
March 28, 2011
What should you tell patients regarding purchase or ingestion of potassium iodide?
With the recent natural disaster in Japan and the resultant damage to the nuclear reactors in Fukushima Daiichi plant, there have been increased concerns about potential radiation exposure in the United States. As a result, there has been increased demand for potassium iodide (KI). KI is used to protect the thyroid from radioactive iodine. The thyroid gland concentrates iodine as it is incorporated into thyroid hormones. Because the thyroid gland can rapidly absorb iodine, including radioactive forms, the thyroid is at risk when there is an exposure to radioactive iodine. Exposure to radioactive iodine can result in long term hypothyroidism, similar to what occurs when patients are given I131 for treatment of hyperthyroidism.
KI is a non-radioactive potassium salt form of iodine. Ingestion of non-radioactive KI prior to exposure to radioactive iodine results in the thyroid gland being “flooded” with the stable form of iodine so the radioactive form is not taken up by the thyroid for the next 24 hours or so. KI does not protect the thyroid if taken after exposure and does not protect other body organs from effects of the radiation. KI also does not protect the body from other forms of radiation.
Currently, there is no expectation that the radiation from the Japanese nuclear power plants will result in harmful exposures in the United States. There is currently no public health concern in the US that would warrant administration of KI. However, some patients are seeking to stockpile or start taking KI. There are three FDA approved formulations of KI. Unfortunately, there are also many websites promoting their unapproved products which could be described as dietary supplements, iodine remedies, sea kelp therapies, etc. If one your patients reports an adverse reaction from either an approved or unapproved product, please advise the FDA through their FDA MedWatch Adverse Event Reporting program: www.fda.gov/MedWatch or calling 800-332-1088.
This question prepared by: Saralyn Williams, MD Medical Toxicologist
-
Question of the Week
January 10, 2011
Are we going to discuss CO exposure again?
Yes we are. This topic was requested by one of our readers and this topic is important enough to discuss every year. This exposure causes unrecognized morbidity and mortality and is one of the most litigated exposures. Never underestimate the impact of CO on your patient or you.
Unfortunately, CO has multiple mechanisms of toxicity and does more than occupy a place on the hemoglobin molecule (carboxyhemoglobin) and create a functional anemia. CO shifts the oxyhemoglobin dissociation curve to the left, so that hemoglobin holds onto oxygen much tighter, reducing the amount of oxygen released to the tissues. CO also causes a malfunction of cytochrome oxidase (oxidizing enzyme in mitochondria which transfers electrons from cytochromes to oxygen molecule) which may last for up to three days after a single exposure. The organ systems most impacted by CO exposure are the heart and nervous system.
The symptoms of CO poisoning are nonspecific and frequently described as “flu-like”. Headache, myalgia, and dizziness may be initial symptoms. Cerebral impairment, confusion, coma and death may subsequently occur. One of the consequences of exposure to CO may be delayed (or persistent) neuropsychological (NP) sequelae which includes memory and concentration impairment, loss of executive function, decrease in IQ, personality changes, neurologic deficits (such as incontinence) and symptoms of Parkinsons syndrome. The young and the old are the most vulnerable. The memory and concentration deficits, as well as impairment of executive function are diagnosed by formal NP testing done by a neuropsychologist. Bedside tests are not sensitive enough to identify these cognitive losses.
The problem is neither the carboxyhemoglobin (COhgb) concentration nor the clinical presentation at the time of evaluation predicts who will develop this sequelae. Not only are we unable to predict who will prevent NP sequelae, but we don’t know if any treatment will prevent or ameliorate the sequelae.
Studies are conflicting regarding the efficacy of hyperbaric oxygen (HBO) and/or normobaric oxygen in preventing or improving this syndrome. There is the possibility that HBO may increase CNS free radicals-although the clinical implications of this are unknown. There are no conclusive studies. There is agreement that HBO is a reasonable treatment for pregnant women as fetal hemoglobin has a higher affinity for CO than adult hemoglobin. Tennessee Poison Center recommends HBO for pregnant women. For other significant exposures, TPC usually recommends 100% oxygen via face mask for at least 12 hours, sometimes longer. Patients with more severe exposures are admitted for 24 hours of 100% oxygen. Most patients are referred for NP testing and then followed up by a toxicologist.
Recommendation: In cases of CO exposure, call the Poison Center, document that you called the PC and their recommendations. These recommendations vary between poison centers. Know what your PC recommends. AND tell all your patients to have a CO detector in their house. Prevention of the exposure is easier than treatment of the sequelae.
This question prepared by: Donna Seger, MD Medical Toxicologist
-
Question of the Week
January 11, 2010
What do you need to know about Carbon Monoxide (CO) exposure?
This is a topic we discuss every year because CO exposure has potential for devastating sequela.
At one time CO was thought to simply occupy a place on the hemoglobin molecule (carboxyhemoglobin) and create a functional anemia. Unfortunately, CO has additional mechanisms of toxicity. CO shifts the oxyhemoglobin dissociation curve to the left, so that hemoglobin holds onto oxygen much tighter, reducing the amount of oxygen released to the tissues. CO also causes a malfunction of cytochrome oxidase (oxidizing enzyme in mitochondria which transfers electrons from cytochromes to oxygen molecule) which may last for up to three days after a single exposure. The organ systems most impacted by CO exposure are the heart and nervous system.
The symptoms of CO poisoning are nonspecific. Headache, myalgia, and dizziness may be initial symptoms. Cerebral impairment, confusion, coma and death may subsequently occur. One of the consequences of exposure to CO may be delayed (or persistent) neuropsychological sequela which includes memory and concentration impairment, loss of executive function, decrease in IQ, personality changes, neurologic deficits (such as incontinence) and symptoms of Parkinsons syndrome. The problem is neither the carboxyhemoglobin (COhgb) concentration nor the clinical presentation at the time of evaluation predicts who will develop this sequelae.
Studies are conflicting regarding the efficacy of hyperbaric oxygen (HBO) and/or normobaric oxygen in preventing or improving this syndrome. There is the possibility that HBO may increase CNS free radicals-although the clinical implications of this are unknown. There are no conclusive studies. There is agreement that HBO is a reasonable treatment for pregnant women as fetal hemoglobin has a higher affinity for CO than adult hemoglobin. Tennessee Poison Center recommends HBO for pregnant women. For other significant exposures, TPC usually recommends NBO for at least 12 hours, sometimes longer.
Recommendation: In cases of CO exposure, call the Poison Center, document that you called the PC and their recommendations. These recommendations will vary between poison centers. Know what your PC recommends. AND tell all your patients to have a CO detector in their house. Prevention of the exposure is easier than treatment of the sequelae.
This question prepared by: Donna Seger, MD Medical Toxicologist
-
Tough Question. In the 1980s it was assumed that CO bound to the hemoglobin molecule and created a functional anemia. Once the CO was gone, everything was fine as long as anoxia hadn�t occurred during the time the CO was attached to hgb. However, in
Korea The memory and concentration deficits, as well as impairment of executive function are diagnosed by formal NP testing done by a neuropsychologist. Bedside tests are not sensitive enough to delineate these cognitive losses.
The problem is, we don�t know who will develop delayed NP sequelae. And, we don�t know if any treatment will prevent or ameliorate it.
There has been a great deal of controversy regarding the use of hyperbaric oxygen (HBO) vs. normobaric oxygen in CO exposed patients. Studies are conflicting- one study implies HBO improves NP outcome compared to NBO and another study implies that NBO improved NP outcome compared to HBO, theoretically due to the HBO-induced generation of free radicals. What a mess.
Our approach at the TN Poison Center is to put all acute CO exposed patients on face mask (100% O2) for 12 hours. For the asymptomatic or minimally symptomatic patients whose symptoms resolve in 12 hours, no further treatment is recommended. Patients with more severe symptomatology or symptoms that don�t resolve, are admitted for 24 hours and 100% O2 normobaric oxygen therapy is continued. HBO is recommended for pregnant women due to the prolonged binding of fetal hgb to CO. A physician is called regarding any significant CO exposures. A Poison Specialist or Medical Toxicologist would be happy to discuss any patients you see with CO exposure.
Question prepared by: Donna L. Seger, M.D. Medical Toxicologist
-
There are 3 types of carbon monoxide detection sensors: biomimetic, semiconductor, and electrochemical. Biomimetic sensors use color change in the presence of the gas for detection. Semiconductors measure change in resistance in a silicon chip when the gas is present. Electrochemical sensors send an electronic signal when a chemical reaction occurs in the presence of carbon monoxide.
While all these systems will detect CO, electrochemical sensors are the most accurate and sensitive of the detectors and are used in professional equipment. These are commonly found in relatively inexpensive detectors for purchase such as those from First Alert. The life of an electrochemical sensor is typically 3 � 5 years.
Because carbon monoxide is lighter than air, detectors should be located at least 5 feet above the ground. They should also be placed at least 10 � 20 feet away from furnaces or other fuel burning sources and 10 feet away from high humidity areas such as bathrooms. The alarm limits of detectors are set at relatively high levels to prevent false alarms such as those caused by cigarette smoke, so when an alarm sounds, it is best to move quickly to a well ventilated area or outside and to contact emergency personnel.
The above question was answered by Mark J. Bogard, CIH, Vanderbilt Environmental Health & Safety/ Chemical Safety Section
We had so many questions about CO detectors that it became necessary to track down an expert. Thanks to Mark Bogard! CDC web sites recommend that the product has the UL seal on it, has some type of battery back up and is used according to the directions.
A recent article in Consumers Reports indicated that less than 50% of homes contain CO detectors. What a potential for disaster! Educate your patients.
-
Why should you have a carbon monoxide detector in your home?
Carbon monoxide (CO) is an odorless, nonirritating gas that is a by-product of incomplete burning of carbonaceous material. CO poisoning may be lethal and even if the exposure is nonfatal, may also result in permanent disability. CO poisoning is considered one of top causes of accidental poisoning death in the
United States CO binds with a high affinity to hemoglobin, thus making the hemoglobin unable to carry oxygen. In addition, CO shifts the oxyhemoglobin curve to the left which reduces oxygen release to the tissues. Thus there is a reduction in the oxygen carrying capacity of the blood; however, this is not the only mechanism of toxicity. CO binds to other heme proteins such as myoglobin and cytochrome oxidase resulting in disruption of cellular respiration. CO increases the production of free radicals, which may result in delayed neurologic sequelae which can result in severe impairments.
CO has no warning properties prior to onset of symptoms from its tissue effects. These symptoms are nonspecific and are usually perceived as a flu-like illness or food poisoning. Use of a functioning CO detector in the home may provide early warning of elevated levels of CO, before significant toxicity occurs. The source of the elevated CO level can then be identified and repaired.
Most smoke detectors, which are more routinely found in homes, do not provide monitoring of CO levels.
Question prepared by: Saralyn R. Williams, M.D. Medical Toxicologist
In the Poison Center Hotline, we have received calls from physicians regarding patients who have been using generators in the house during our recent cold snap. Entire families have been exposed to carbon monoxide. A number of television stations in TN and
Kentucky
-
TVA Roane County Fly Ash Disaster - What happened and what it means?
The TVA Kingston Fossil Plant produces fly ash as a result of burning coal to create electricity. Fly ash is the leftover ash from the power generating plant. In order to reduce air pollution, the air being released through the smokestacks is �scrubbed to capture the fly ash waste. This is �wetted (mixed with water) and then kept in retention ponds on site. Due to heavy rains, one of the dikes containing an 80 acre pond with fly ash sludge broke on December 22, 2008 just before 1 am. This ash-slide covered an estimated area of 250-400 acres and was up to 4-6 feet deep.
No human injuries occurred as a result of this collapse but about 15 homes were affected, including one that was pushed from its foundation. A gas line was ruptured, a road was blocked and power lines were downed in this event. A train delivering coal to the plant was also affected.
TVA along with TN Department of Environmental Conservation and US EPA immediately responded. Families were evacuated, barriers were erected to limit spread of ash-slide and water flows were reduced downstream to limit the spread of ash. Water sampling from private wells is occurring within a 4 mile radius of the release as well as river water sampling of the rivers involved (Emory and
Tennessee From the
Tennessee Poison Center Here are some additional resources for further information on this disaster:
Tennessee Valley Authority
Public outreach - 865-632-1700
Property damage assessments - 1-800-257-2675
Media - 865-590-7001 or 865-632-6000
Tennessee Department of Environment and Conservation
Public - 888-891-8332 or ask.tdec@state.tn.us
Media - Tisha Calabrese-Benton 865-594-5442 or
tisha.calabrese@state.tn.us
Meg Lockhart 615-253-1916 or
meg.lockhart@state.tn.us
Tennessee Department of Health
Public - 1-800-404-3006 or Roane County Health Department at
865-354-1220
Media - 615-741-3111
Tennessee Wildlife Resources Agency
Public/Media - Dan Hicks - 1-800-262-6704
U.S. Environmental Protection Agency
Public - 1-800-241-1754 or 404-562-9900
Media - 404-562-8327
Roane County
Public - 865-717-4212 or email:
tvarecovery@roanegov.org
Media - 865-717-4440 or
scottstout@roanegov.org
Tennessee Emergency Management Agency
Public - 1-800-262-3300
Media - 615-741-0482Question prepared by: John G. Benitez, M.D., MPH Medical Toxicologist