
Testimony of Dr. Melinda Buntin regarding HB0278 and on the Topic of All-Payer Claims Databases
Note: Testimony was given before the Tennessee General Assembly House Insurance Committee April 15, 2019.
Thank you Chairman Travis, Chairman Daniel, and members of the Insurance committee. I am delighted to be here today to talk about the benefits of an All-Payer Claims Database (APCD) to the people and state of Tennessee. My name is Melinda Buntin and I am a health economist and Professor at Vanderbilt School of Medicine. Today, I am speaking in my role as a health economist, and not as a representative of Vanderbilt University or Vanderbilt University Medical Center.
As health economist, I can say that All-Payer Claims Databases are a key part of efforts to promote transparency, competition, consumer engagement in health care, and better value in a growing number of states across the country.
First, what is an all-payer claims database?
- An APCD is a large, state-sponsored database that usually includes medical, pharmacy, and dental claims, as well as eligibility files collected from private and public payers.[i]
- APCD data are reported directly by insurers to states, usually as part of a state mandate.
- 3 main advantages of APCDs over other available datasets:[ii]
- Includes private insurer information that many other datasets do not.
- Includes data from most or all insurance companies in a particular state, in contrast to some proprietary datasets.
- Includes information on care for patients across care sites, rather than visits reported as discharge data.
Also includes over-time information with large sample sizes, geographic representation, and capture of longitudinal information on individual patients while preserving patient confidentiality.
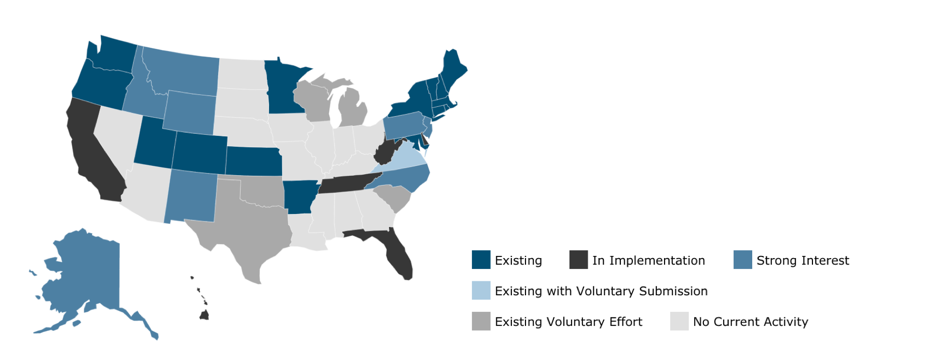
- More than 20 states have invested in implementing statewide APCDs.
What can you do with an all-payer claims database?
- Assess variation in price and utilization across providers, insurers and geographic areas. Also allows tracking healthcare spending drivers and trends.
- MA APCD data has been used to produce annual report of trends in healthcare spending for commercial payers versus Medicaid by service category, episode type, and geographic area. Credited with helping to keep health care cost increases low.
- Promote public health
- VA, AK, and UT organizations have used APCD data to track opioid prescription and claims – can look at clinical context and patient characteristics to understand and address trends.
- TN State Department of Health doing an excellent job by looking at payers of providers and patients, but can’t understand the clinical context in which an opioid prescription is written with the data currently available.
- Assess the impact of policy changes
- Arkansas Center for Health Improvement has used their APCD to investigate:
- Increases in Epipen prices
- Balance billing liability for air ambulance, which has also been a problem in Tennessee
- Differences in payments for flu vaccines between Medicaid and private insurance to understand why providers weren’t providing flu vaccines to Medicaid patients.
- Arkansas Center for Health Improvement has used their APCD to investigate:
- Make provider-level price and quality information available to consumers, health plan enrollees, and employers to promote cost transparency.
- New Hampshire, Maine, Maryland have healthcare transparency websites that let you compare the costs of common procedures by facility, provider, and insurer.[ii]
- In Maine, more than 50,000 consumers used the database. The procedures that were most frequently researched were deliveries, colonoscopies, and knee and hip replacements.
- Director of CompareMaine.org (Maine’s APCD) – Legislators thank her for saving constituents hundreds of dollars and constituents are very appreciative of tools made available by the state.
Coverage in APCDs:
- Arkansas’ APCD includes 85% of their market.
- Maine’s APCD covers 87% of their market.
- Regarding ERISA Plans: A 2016 Supreme Court ruling (Gobeille v. Liberty Mutual Insurance Co., Inc.) stated that ERISA plans could not be compelled to provide data to a state-sponsored APCD. However, many states have asked for voluntary participation for large employers, and many large employers are very happy to contribute because it makes them a better manager of their benefits. Medicare also tends to participate.
Other Innovative Uses of APCDs
- Minnesota: examining Opioid prescribing patterns and new chronic opioid users
- ACPD data provide unique insight into details about prescription opioid use and prescribing patterns, as well as richer clinical contextual information about prescribing patterns
- Vermont: Using VT Healthcare Claims Uniform Reporting and Evaluation System (VHCURES, their APCD) to find trends in health care service expenditures and utilization with a statewide expansion of opioid use disorder treatment using a medication-assisted treatment system[iv]
- Membership trends, demographics, expenditures and treatment costs, ED and inpatient discharges, linked claims and incarceration data, etc.
- Colorado: Center for Improving Value in Health Care (a not-for-profit organization) began collecting claims data in early 2012 as a part of efforts to “improve the health of all Coloradans”, and achieved Triple Aim of better health, better health care, and lower costs.[v]
‘Right to Shop’ Laws and APCDs
- Give patients the ability to benefit financially when they choose lower-cost care.[vi]
- For example, New Hampshire consumers receive a share of the savings in cash if they select a provider/service with a lower price. Maine has transparency provisions that require insurers to give patients anticipated charges and estimated out-of-pocket charges before receiving care.
- Similar to the idea of a transparency website built on APCD, but a successful implementation of Right to Shop laws will require comprehensive databases, like an APCD.
[iv] OUD and Treatment Research in VHCURES, Vermont’s All-Payer Claims Database. Blueprint for Health. November 14, 2018. https://www.apcdcouncil.org/sites/default/files/media/2019.2.21.mohlman.apcd_opioid_research.pdf
[v] Realizing the Potential of All-Payer Claims Databases. Green L, Lischko A, Bernstein T. RWJF. January 14, 2014. https://www.rwjf.org/en/library/research/2014/01/realizing-the-potential-of-all-payer-claims-databases--creating-.html
[vi] Right to Shop: The next big thing in health care. Josh Archambault. Forbes. August 5, 2016. https://www.forbes.com/sites/theapothecary/2016/08/05/right-to-shop-the-next-big-thing-in-health-care/#bd752ca4f601