TOXICOLOGY QUESTION OF THE WEEK
October 6, 2023
What causes acute hypertension, tachycardia, and pulmonary edema in a 40-year-old male?
For the next couple of weeks, I am going to discuss cases presented by Tox Fellows at the monthly National Case Conference. I’ve used case presentations from this venue in previous years and discovered that the readership finds them as fascinating as I do.
Case: A 40-year-old male presents to the ED with shortness of breath and increased work of breathing. Vital signs: HR 120, BP 150/90, RR 30 afebrile. O2 sat 89% on RA which increases to 94% on 4 L oxygen. He is unable to lie flat.
Only medication is propranolol which he takes for palpitations and tachycardia. He is a body builder and follows a bodybuilding diet.
CXR-pulmonary edema: EKG: deeply inverted T waves (? Ischemic changes)
AG-12; Ca-9.6 mg/dL; Troponin 374 ng/mL; rest of lab wnl
ECHO LVH with 10% EF
Diff Dx discussion: GHB withdrawal (GHB frequently used in body building); Takotsubo cardiomyopathy (wall motion abnormality in LV associated with stress); Anabolic androgenic steroids (AAS) causing myocarditis; Wellens syndrome (inverted Ts in V2 and V3 indicative of stenosis in LAD); pulmonary embolus, high output failure secondary to thyrotoxicosis.
Cardiology C/S-acute decompensated heart failure. Diuresis initiated.
DX: AAS(patient finally admitted to long term steroid use) ingestion causing cardiomyopathy and heart failure
The patient responded well to treatment.
Notes:
Definition: anabolic-skeletal muscle building properties; androgenic-induction and maintenance of secondary male sexual characteristics.
Testosterone is the primary endogenous hormone belonging to this class of drugs.
AAS are easily obtained from local dealers or the internet.
Pharmacokinetics: Rapidly absorbed after oral ingestion with peak concentration peaking 1-2 hours after ingestion of methyltestosterone. A large fraction of the AAS is metabolized by the liver (first pass metabolism), reducing the bioavailability before entering the circulation. For example, oral administration of 25 mg testosterone only results in 1 mg entering the systemic circulation. IM administration results in much better bioavailability (bypasses first pass metabolism by the liver.) From the bloodstream, AAS move into extravascular compartments and undergo biotransformation or bind to the testosterone receptor. (Ref 3 is a great overview of pharmacokinetics and side effects.)
AAS Clinical effects and potential toxicity (see figure): Virilization, cholestatic hepatitis depression, anxiety, mania, psychosis, excess sweating, hypertension, acne, hyperlipidemia, erythrocytosis, Cardiomyopathy and Heart Failure
Steroid Jargon:
Cycling: taking multiple doses over a specific period of time then stop then start again
Stacking; taking 2 or more steroids
Pyramiding: start with low dose, increase frequency or number of pills then taper in cycles
Plateauing: changing to another steroid suddenly to keep steroid from becoming ineffective then switching back to original steroid
REFERENCES
1) Ahlgrim C, Guglin M.J Anabolics and cardiomyopathy in a bodybuilder: case report and literature review. Card Fail. 2009 Aug;15(6):496-500. doi: 10.1016/j.cardfail.2008.12.014. Epub 2009 Feb 10.PMID: 19643360 Review.
2) De Turck L, Sarens T, Veldeman L, Vonck A. For the love of muscles: a bodybuilder with complicated left ventricular heart failure. Acta Cardiol. 2022 Nov;77(9):774-777. doi: 10.1080/00015385.2022.2080919. Epub 2022 Aug 16. PMID: 35972452.
3) Bond P, Smit DL, de Ronde W. Anabolic-androgenic steroids: How do they work and what are the risks? Front Endocrinol (Lausanne). 2022 Dec 19;13:1059473. doi: 10.3389/fendo.2022.1059473. PMID: 36644692; PMCID: PMC9837614.
Question submitted by Donna Seger MD
Comment: A presentation of pulmonary edema does not usually cause the ingestion of anabolic steroids to jump to mind. This case demonstrates the need to always ascertain hobbies and use of supplements or herbals. Some toxin-induced cardiomyopathies get better. The outcome of this case is still unknown, but he did respond well to the treatment of pulmonary edema.
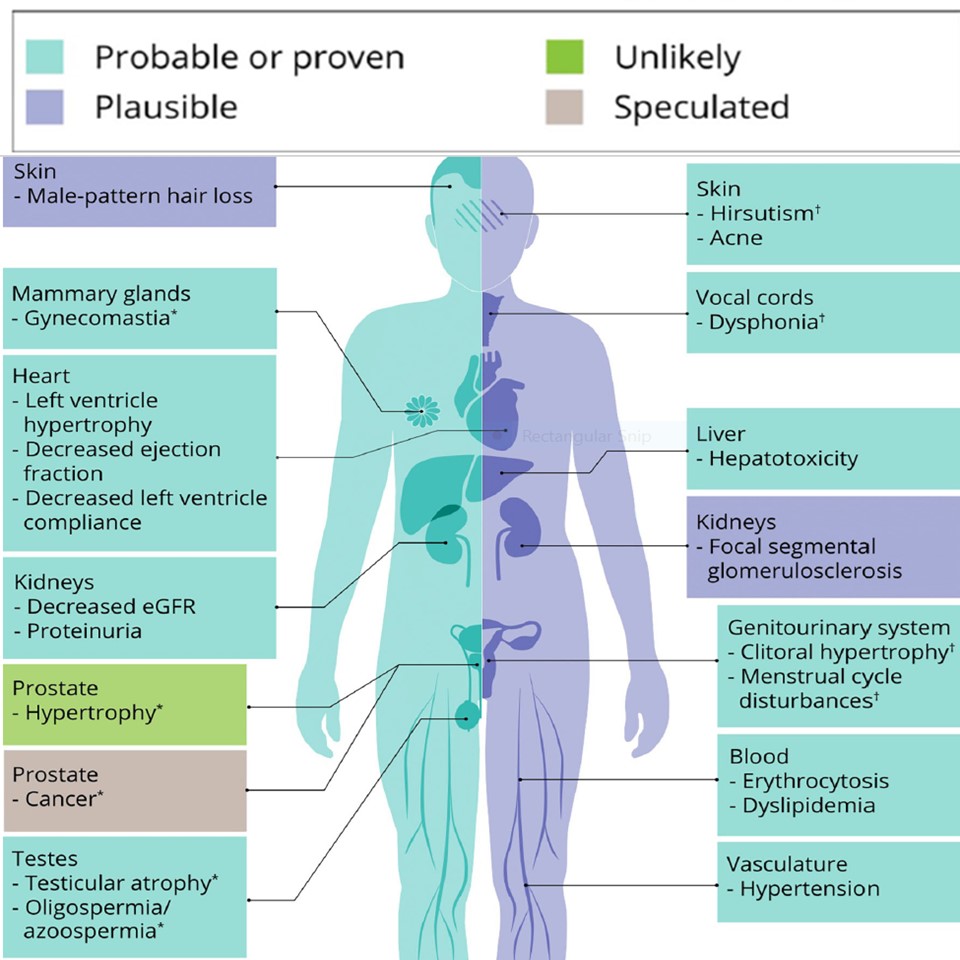
Side effects of anabolic androgenic steroids (reference 3)
I am interested in any questions you would like addressed in the Question of the Week. Please email me with any suggestions at donna.seger@vumc.org.
DONNA SEGER, MD
Professor Emeritus
Department of Medicine
VUMC
|
|
TENNESSEE POISON CENTER 24/7 FREE MEDICAL HOTLINE
POISON HELP | 800.222.1222
|

